

Welcome to the new page: Neuropsychology. I personally consider it one of the most fascinating areas in Psychology, and I really hope you will regard it as such as well after going through the the presented posts.
To begin with, I will do a couple of articles which will cover the basics of neuropsychology, mainly theory, methodology and overview of key neuropsychological disorders. Later on I will make sure that the page develops and grows further, together with this relatively young discipline.
In the current post I will discuss the main issues and questions posed by neuropsychologists, and will also talk about the methods used in the field, including case (lesion) studies, group (behavioural) studies and different types of brain imaging.
To begin with, I will do a couple of articles which will cover the basics of neuropsychology, mainly theory, methodology and overview of key neuropsychological disorders. Later on I will make sure that the page develops and grows further, together with this relatively young discipline.
In the current post I will discuss the main issues and questions posed by neuropsychologists, and will also talk about the methods used in the field, including case (lesion) studies, group (behavioural) studies and different types of brain imaging.
Key questions
So what are the basic questions of neuropsychology?
1. Question of functional localisation: can mental functions be dissociated from one another? In other words, is our ability to perform task A related to our ability to perform task B?
2. Question of anatomical localisation: can mental functions be localised in separate brain areas? Is each of the brain areas responsible for a particular function/ability?
3. How do brain functions interact if they do?
4. Plasticity issue: are these functions modifiable and compensatory?
5. Role of genes and environment on anatomy and function of the brain.
These are very broad questions, but essentially they underpin the majority of research in neuropsychology.
1. Question of functional localisation: can mental functions be dissociated from one another? In other words, is our ability to perform task A related to our ability to perform task B?
2. Question of anatomical localisation: can mental functions be localised in separate brain areas? Is each of the brain areas responsible for a particular function/ability?
3. How do brain functions interact if they do?
4. Plasticity issue: are these functions modifiable and compensatory?
5. Role of genes and environment on anatomy and function of the brain.
These are very broad questions, but essentially they underpin the majority of research in neuropsychology.
Modularism

Franz Joseph Gall
| The idea of modularity of mind was first proposed by Franz Joseph Gall, founder of phrenology. His basic idea was that mental capacity consisted of separable functions, which can be located in separable brain areas (thus he supported the idea of anatomical localisation). | 
Phrenology map
|
Gall also believed that when a certain function is used, the corresponding brain region grows in size; thus, the more person uses a particular function more frequently than others, detectable lumps develop in a skull; analysis of these then can 'tell' you which brain area is responsible for which function. To him, because each mental function corresponded with an area in the brain, you could literally 'read off' one's level of intelligence or talents from the sizes of lumps and bumps on the person's skull.
Of course, Gall got it really wrong about the lumps. The idea did not live long, and was discredited after the head of a composer Joseph Haydn was stolen after his burial in 1809 by two phrenologists, who wanted to study it and locate the brain areas responsible for musicality. Scandal!
However, in the 1980s Jerry Fodor revived the idea of modularity of mind, leaving out the physical correspondence to mental functions. The important alteration to the previous idea was that the functions were no longer seen as necessarily domain-specific, and mental processes were now understood as interactions between different faculties (or, cognitive modules) such as memory, imagination etc. Thus, Fodor argued in favour of functional localisation rather than anatomical one.
Fodor's theory also included the notion that lesions disrupt specific modules in the brain, and so, the brain with lesion could be described as: normal brain minus the affected region. This idea, however, has been disproven, as several studies showed that the brain is able to compensate for the lost modules, 'moving' lost function to a different brain region.
The theory of modularism proved to be very influential, and has guided the brain studies since 1980s. Now I would like to discuss the methods which neuropsychologists use in order to test the theory and study the modularity of the brain.
Of course, Gall got it really wrong about the lumps. The idea did not live long, and was discredited after the head of a composer Joseph Haydn was stolen after his burial in 1809 by two phrenologists, who wanted to study it and locate the brain areas responsible for musicality. Scandal!
However, in the 1980s Jerry Fodor revived the idea of modularity of mind, leaving out the physical correspondence to mental functions. The important alteration to the previous idea was that the functions were no longer seen as necessarily domain-specific, and mental processes were now understood as interactions between different faculties (or, cognitive modules) such as memory, imagination etc. Thus, Fodor argued in favour of functional localisation rather than anatomical one.
Fodor's theory also included the notion that lesions disrupt specific modules in the brain, and so, the brain with lesion could be described as: normal brain minus the affected region. This idea, however, has been disproven, as several studies showed that the brain is able to compensate for the lost modules, 'moving' lost function to a different brain region.
The theory of modularism proved to be very influential, and has guided the brain studies since 1980s. Now I would like to discuss the methods which neuropsychologists use in order to test the theory and study the modularity of the brain.
Methods of Neuropsychology
One way of categorising neuropsychological studies is by single case studies (lesion studies) and group studies. The single case studies help to pick out possible functional associations and dissociations in mental functions. They often help to develop a theory or an idea, which is then developed by looking at groups of patients with the same symptoms - or those showing potential double dissociations (read on associations and dissociations here).
Other methods of neuropsychology include brain imaging which can be divided into:
1. Event-related potentials (ERPs)
ERP is a measured brain response to a specific sensory, cognitive or motor stimuli. Its big plus is that it is a non-invasive way of evaluating activity and functioning of the brain. It is also much cheaper than inserting microelectrodes and using fMRI and PET. However, it only produces temporal, but not spacial resolutions. In other words, it can show very precisely when brain activates - however not where it activates.
2. Structural neuroimaging
Structural imaging allows to take a 'picture' of a brain using magnetic fields and radio waves (e.g. MRI, CT). It allows us to see the density of the brain's matter; the denser the area is, the whiter it will appear on the scan. It allows neurologists to see the potential tumours or losses of grey matter.
3. Functional neuroimaging
Functional neuroimaging allows to detect the blood flow to measure neural activity (fMRI, PET). It produces a series of 'colourful' pictures, colours reflecting the changes in blood flow.
Other methods of neuropsychology include brain imaging which can be divided into:
1. Event-related potentials (ERPs)
ERP is a measured brain response to a specific sensory, cognitive or motor stimuli. Its big plus is that it is a non-invasive way of evaluating activity and functioning of the brain. It is also much cheaper than inserting microelectrodes and using fMRI and PET. However, it only produces temporal, but not spacial resolutions. In other words, it can show very precisely when brain activates - however not where it activates.
2. Structural neuroimaging
Structural imaging allows to take a 'picture' of a brain using magnetic fields and radio waves (e.g. MRI, CT). It allows us to see the density of the brain's matter; the denser the area is, the whiter it will appear on the scan. It allows neurologists to see the potential tumours or losses of grey matter.
3. Functional neuroimaging
Functional neuroimaging allows to detect the blood flow to measure neural activity (fMRI, PET). It produces a series of 'colourful' pictures, colours reflecting the changes in blood flow.
fMRI imaging
Chromo-phrenology?
Functional neurimaging is a great technique of course - however, it has been referred to as 'chromo-phrenology', with the meaning that it brings back the same old idea of phrenology (i.e. aims to divide the brain into simplistic, separable areas corresponding to mental functions) just making it a bit more fancy, adding some nice colours. A great research done by D. Weisberg et al. (2008) demonstrated that people were much more likely to trust a psychological study if there were some brain imaging pictures included as an evidence - even in cases when the scans were absolutely irrelevant to arguments. The paper is now in a public domain and can be found here: 'The Seductive Allure of Neuroscience Explanation'.
There are many other limitations of brain imaging which those studying neuropsychology should be aware of. fMRI measures blood flow, therefore it is an INdirect measurement of neural activity. This is important to remember, as this fact brings out many potential problems:
1. Change in blood flow may demonstrate inhibition as well as activation of the area.
2. There are a lot of individual differences when it comes to brain structure, which can make it hard to interpret functional scans. Here, for example, is a topography of Brodmann area 41 in 9 different subjects; all the scans show quite a different structure and localisation of the area:
There are many other limitations of brain imaging which those studying neuropsychology should be aware of. fMRI measures blood flow, therefore it is an INdirect measurement of neural activity. This is important to remember, as this fact brings out many potential problems:
1. Change in blood flow may demonstrate inhibition as well as activation of the area.
2. There are a lot of individual differences when it comes to brain structure, which can make it hard to interpret functional scans. Here, for example, is a topography of Brodmann area 41 in 9 different subjects; all the scans show quite a different structure and localisation of the area:
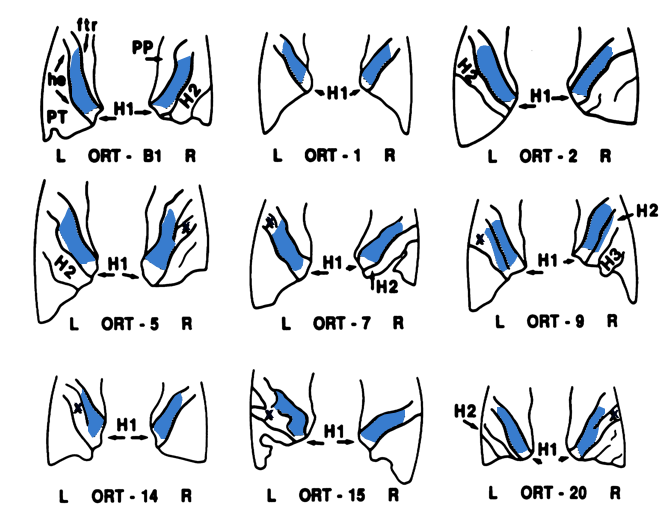
Brodmann area 41. From Rademacher, Caviness, Steinmetz, & Galaburda, 1993
3. Activation of a certain area does not necessarily mean that it is dedicated SOLELY to the performed function. In fact, it does not even mean that it is necessary for the function at all, and could have been activated for numerous other reasons.
4. At the same time, the lack of activation is also ambiguous as it could mean either subliminal (i.e. very weak, undetectable) activation or, indeed, permanent activation, as fMRI only detects changes in blood flow.
4. At the same time, the lack of activation is also ambiguous as it could mean either subliminal (i.e. very weak, undetectable) activation or, indeed, permanent activation, as fMRI only detects changes in blood flow.
 RSS Feed
RSS Feed
