

The first one to identify, study and record a thought disorder was Emil Kraepelin, who called it dementia praecox (premature dementia). Among the symptoms he listed hallucinations, social withdrawal, apathy, indifference and lost capacity to function normally. It was renamed to schizophrenia by a Swiss psychiatrist Paul Eugen Bleuler (from the Greek 'skhizein' = 'split' and 'phren' = 'mind').
Today I will discuss the prevalence, subtypes, risk factors and treatment employed in cases of schizophrenia.
Today I will discuss the prevalence, subtypes, risk factors and treatment employed in cases of schizophrenia.
Schizophrenia
Saha et al. (2005) studied 188 cases across 46 countries and found that schizophrenia is prevalent in 0.16-1.2% of society with no gender differences. They also found that it is roughly 1.8 times more frequent in immigrants than in the native born, and that the prevalence was lower in less developed countries. Gorwood et al., 1995, showed that the age of onset is about 27.8 in men and 31.8 in women, however this difference disappeared in cases with family history.
According to the last edition of Diagnostic and Statistical Manual of Mental Disorders (DSM), a person is diagnosed with schizofrenia if at least two of the following symptoms are apparent for at least one month:
- Delusions
- Hallucinations
- Disorganised speech
- Disorganised and Catatonic behaviour
- Negative symptoms
Delusions are present in about 90% of the cases. These are erroneous, irrational beliefs which are held very strongly by a person. For example, in case with paranoid schizophrenia (I will discuss it further down), patients believe that they are being watched by others (sometimes even with the use of hidden cameras); that others want to harm them, etc. One of the most frequent ones is delusion of grandeur: when a person considers him/herself more powerful or somehow better than others; that (s)he is invincible etc.
Hallucinations are mostly auditory (75%), but might be visual as well (around 15% of cases). Tactile and other hallucinations are much rarer. Auditory hallucinations typically feature voices which either threaten or control the patient. It is often a voice of someone patient knows, but can be an abstract one too, as well as one of God, devil etc. In 1996, Nayani and David interviewed schizophrenics with auditory hallucinations and found out that the voices were mostly speaking in a conversational volume but almost always were rude and vulgar.
Schizophrenics often experience disordered speech: speech which is correct grammatically, but does not make sense content-wise, as it is incoherent, with weak associations and with a frequent presence of neologisms.
Disorganised behaviour affects person's ability to perform everyday routine, and includes poor personal hygiene, disregard to personal safety, unusual choice of clothes etc. Catatonic behaviour (catatonia) is a absence of movement or/and speech. Those with catatonia hold certain body positions for a long period of time, like a statue.
Negative symptoms refer to the absence of behaviours which are normally present (behaviour without a goal, difficulty concentrating, distorted speech etc.).
According to the last edition of Diagnostic and Statistical Manual of Mental Disorders (DSM), a person is diagnosed with schizofrenia if at least two of the following symptoms are apparent for at least one month:
- Delusions
- Hallucinations
- Disorganised speech
- Disorganised and Catatonic behaviour
- Negative symptoms
Delusions are present in about 90% of the cases. These are erroneous, irrational beliefs which are held very strongly by a person. For example, in case with paranoid schizophrenia (I will discuss it further down), patients believe that they are being watched by others (sometimes even with the use of hidden cameras); that others want to harm them, etc. One of the most frequent ones is delusion of grandeur: when a person considers him/herself more powerful or somehow better than others; that (s)he is invincible etc.
Hallucinations are mostly auditory (75%), but might be visual as well (around 15% of cases). Tactile and other hallucinations are much rarer. Auditory hallucinations typically feature voices which either threaten or control the patient. It is often a voice of someone patient knows, but can be an abstract one too, as well as one of God, devil etc. In 1996, Nayani and David interviewed schizophrenics with auditory hallucinations and found out that the voices were mostly speaking in a conversational volume but almost always were rude and vulgar.
Schizophrenics often experience disordered speech: speech which is correct grammatically, but does not make sense content-wise, as it is incoherent, with weak associations and with a frequent presence of neologisms.
Disorganised behaviour affects person's ability to perform everyday routine, and includes poor personal hygiene, disregard to personal safety, unusual choice of clothes etc. Catatonic behaviour (catatonia) is a absence of movement or/and speech. Those with catatonia hold certain body positions for a long period of time, like a statue.
Negative symptoms refer to the absence of behaviours which are normally present (behaviour without a goal, difficulty concentrating, distorted speech etc.).
Subtypes
1. Paranoid schizophrenia
The most common subtype. The defining feature is auditory hallucinations or persistent delusional thoughts about persecution or conspiracy. However, people with this subtype may be more functional in their ability to work and engage in relationships than people with other subtypes of schizophrenia. Since there may be no observable features, the evaluation requires sufferers to be somewhat open to discussing their thoughts. If there is a significant degree of suspiciousness or paranoia present, people may be very reluctant to discuss these issues with a stranger.
2. Disorganised subtype
Predominant feature is disorganisation of the thought processes. Typically, hallucinations and delusions are less pronounced. These people may have significant impairments in their ability to maintain the activities of daily living. Even the more routine tasks, such as dressing, bathing or brushing teeth, can be significantly impaired or lost. Often, there is impairment in the emotional processes of the individual. For example, these people may appear emotionally unstable, or their emotions may not seem appropriate to the context of the situation.
3. Undifferentiated subtype
This subtype is characterised with symptoms which are not sufficiently formed or specific enough to permit classification of the illness into one of the other subtypes.
The symptoms of any one person can fluctuate at different points in time, resulting in uncertainty as to the correct subtype classification. Other people will exhibit symptoms that are remarkably stable over time but still may not fit one of the typical subtype pictures.
4. Residual schizophrenia
This subtype is diagnosed when the patient no longer displays prominent symptoms. In such cases, the schizophrenic symptoms generally have lessened in severity. Hallucinations, delusions or abnormal behaviours may still be present, but their manifestations are significantly diminished in comparison to the acute phase of the illness. Just as the symptoms of schizophrenia are diverse, so are its consequences. Different kinds of impairment affect each patient’s life to varying degrees. Some people require custodial care in state institutions, while others are employed and can maintain an active family life. However, the majority of patients are at neither of these extremes. Most will have an unstable course of disorder marked with occasional hospitalizations and some assistance from outside support sources.
5. Catatonic subtype
The predominant feature is disturbance in movement. Affected people may exhibit a dramatic reduction in activity, to the point that voluntary movement stops, as in catatonic stupor. Alternatively, activity can dramatically increase, a state known as catatonic excitement. Se the video below.
The most common subtype. The defining feature is auditory hallucinations or persistent delusional thoughts about persecution or conspiracy. However, people with this subtype may be more functional in their ability to work and engage in relationships than people with other subtypes of schizophrenia. Since there may be no observable features, the evaluation requires sufferers to be somewhat open to discussing their thoughts. If there is a significant degree of suspiciousness or paranoia present, people may be very reluctant to discuss these issues with a stranger.
2. Disorganised subtype
Predominant feature is disorganisation of the thought processes. Typically, hallucinations and delusions are less pronounced. These people may have significant impairments in their ability to maintain the activities of daily living. Even the more routine tasks, such as dressing, bathing or brushing teeth, can be significantly impaired or lost. Often, there is impairment in the emotional processes of the individual. For example, these people may appear emotionally unstable, or their emotions may not seem appropriate to the context of the situation.
3. Undifferentiated subtype
This subtype is characterised with symptoms which are not sufficiently formed or specific enough to permit classification of the illness into one of the other subtypes.
The symptoms of any one person can fluctuate at different points in time, resulting in uncertainty as to the correct subtype classification. Other people will exhibit symptoms that are remarkably stable over time but still may not fit one of the typical subtype pictures.
4. Residual schizophrenia
This subtype is diagnosed when the patient no longer displays prominent symptoms. In such cases, the schizophrenic symptoms generally have lessened in severity. Hallucinations, delusions or abnormal behaviours may still be present, but their manifestations are significantly diminished in comparison to the acute phase of the illness. Just as the symptoms of schizophrenia are diverse, so are its consequences. Different kinds of impairment affect each patient’s life to varying degrees. Some people require custodial care in state institutions, while others are employed and can maintain an active family life. However, the majority of patients are at neither of these extremes. Most will have an unstable course of disorder marked with occasional hospitalizations and some assistance from outside support sources.
5. Catatonic subtype
The predominant feature is disturbance in movement. Affected people may exhibit a dramatic reduction in activity, to the point that voluntary movement stops, as in catatonic stupor. Alternatively, activity can dramatically increase, a state known as catatonic excitement. Se the video below.
Risk Factors
1. Genetic
Multiple studies showed that genes is the strongest predictor of developing the disorder. Concordance studies demonstrated that family history carries the biggest risk; see the full diagram below.
Multiple studies showed that genes is the strongest predictor of developing the disorder. Concordance studies demonstrated that family history carries the biggest risk; see the full diagram below.
Heston, 1966, examined 97 adopted children, 47 born to schizophrenic and 50 - to healthy mothers. He found that 16.6% of children with ill biological mothers developed the disorder later in life, while none of those with healthy mothers did.
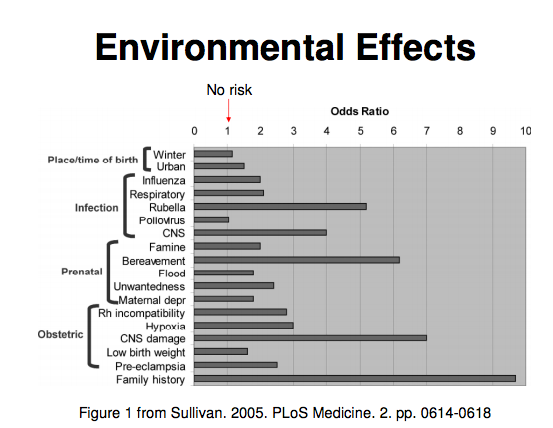
2. Environment
Another adoptive study was conducted by Finnish psychologist Tienari (2004). He looked at the adopted children born to healthy and schizophrenic mothers; he also examined the adoptive family environment and classified it as 'healthy' or 'dysfunctional'. What he found was that children with a healthy biological mother were under the same risk to develop schizophrenia despite the adoptive environment. Children born to a mother with the disorder were under the same risk (5%) if brought up in a healthy environment, however the risk went up to 20% in a 'dysfunctional' one. This means that environment does matter but plays a secondary role.
Below you can find a table which shows the risk which various environmental factors bring; you will find that the family history is still the strongest factor.
2. Environment
Another adoptive study was conducted by Finnish psychologist Tienari (2004). He looked at the adopted children born to healthy and schizophrenic mothers; he also examined the adoptive family environment and classified it as 'healthy' or 'dysfunctional'. What he found was that children with a healthy biological mother were under the same risk to develop schizophrenia despite the adoptive environment. Children born to a mother with the disorder were under the same risk (5%) if brought up in a healthy environment, however the risk went up to 20% in a 'dysfunctional' one. This means that environment does matter but plays a secondary role.
Below you can find a table which shows the risk which various environmental factors bring; you will find that the family history is still the strongest factor.
Drug treatment
Antipsychotics are the drugs typically prescribed to treat schizophrenia. There are typical (first generation, developed in 1950s) and atypical (second generation) antipsychotics. Typical ones block D2 dopamine receptors. They are quite effective in dealing with positive symptoms, however have a lot of side effects including weight gain, drowsiness, reduced motor ability etc. Atypical type blocks a wider range of dopamine receptors and deal with both negative and positive symptoms. However, they are associated with a diabetes risk and drop in white cell amount.
Behavioural therapy
Medications are normally used alongside the cognitive-behavioural therapy. Aim of the therapy is to conduct a reality check together with the patient, and discredit his/her delusional thoughts. The therapy has proved quite successful; also - when used with placebo rather than real medications.
Only about 16% of schizophrenics recover fully, while about 12% require constant hospitalisation and caretaker. 38% or so can function in a society more or less successfully. The mortality rate among schizophrenics is 2-3 times higher than that among healthy people, both due to increased suicide possibility and higher risk of death related to poor self-maintenance (hygiene, safety, etc.).
Only about 16% of schizophrenics recover fully, while about 12% require constant hospitalisation and caretaker. 38% or so can function in a society more or less successfully. The mortality rate among schizophrenics is 2-3 times higher than that among healthy people, both due to increased suicide possibility and higher risk of death related to poor self-maintenance (hygiene, safety, etc.).
 RSS Feed
RSS Feed
