
The basic definition of aphasia is a deficit of language function; the word itself comes from the Greek 'aphatos', literally meaning 'speachlessness'. However, rather than being a uniform impairment, it is a broad term for different types of aphasia, each of which affects certain aspect of language.
In this post, I will talk about what causes aphasia, different types of the condition and some of the treatments of aphasia which are used nowadays.
In this post, I will talk about what causes aphasia, different types of the condition and some of the treatments of aphasia which are used nowadays.
Why?
Aphasia occurs when the language centre of the brain is damaged. The language centre is, however, not a single unit, but consists of a network of brain areas which work together. These include:
- Broca's area: believed to be responsible for producing speech
- Wernicke's area: language comprehension
- Auditory cortex: transforms sounds of speech into meaningful information
- Motor cortex: controls parts of the body used to produce speech such as face and tongue muscles.
We can see that different brain areas are responsible for certain language aspects; however, it does not mean that injury of a specific area would necessarily lead to a 'correspondent' type of aphasia. For example, it is not always the case that the damage of Broca's area causes Broca's aphasia (that is, impairment of language production). Effects of brain damage vary widely across different patients. Also, brain often demonstrates high plasticity, dedicating lost function to a different area.
The brain might get damaged in various ways including the following:
1. Stroke is the most common cause of aphasia; as many as 1/3 of those who had a stroke suffer from aphasia in some form. Stroke occurs when a blood supply to brain cells stops, causing brain cells to die from lack of nutrients and oxygen.
2. Head injury
3. Brain tumour
4. Neurodegenerative diseases, such as dementia and Alzheimer's disease. These cause progressive loss of brain cells, and can cause aphasia if the language centre is affected.
- Broca's area: believed to be responsible for producing speech
- Wernicke's area: language comprehension
- Auditory cortex: transforms sounds of speech into meaningful information
- Motor cortex: controls parts of the body used to produce speech such as face and tongue muscles.
We can see that different brain areas are responsible for certain language aspects; however, it does not mean that injury of a specific area would necessarily lead to a 'correspondent' type of aphasia. For example, it is not always the case that the damage of Broca's area causes Broca's aphasia (that is, impairment of language production). Effects of brain damage vary widely across different patients. Also, brain often demonstrates high plasticity, dedicating lost function to a different area.
The brain might get damaged in various ways including the following:
1. Stroke is the most common cause of aphasia; as many as 1/3 of those who had a stroke suffer from aphasia in some form. Stroke occurs when a blood supply to brain cells stops, causing brain cells to die from lack of nutrients and oxygen.
2. Head injury
3. Brain tumour
4. Neurodegenerative diseases, such as dementia and Alzheimer's disease. These cause progressive loss of brain cells, and can cause aphasia if the language centre is affected.
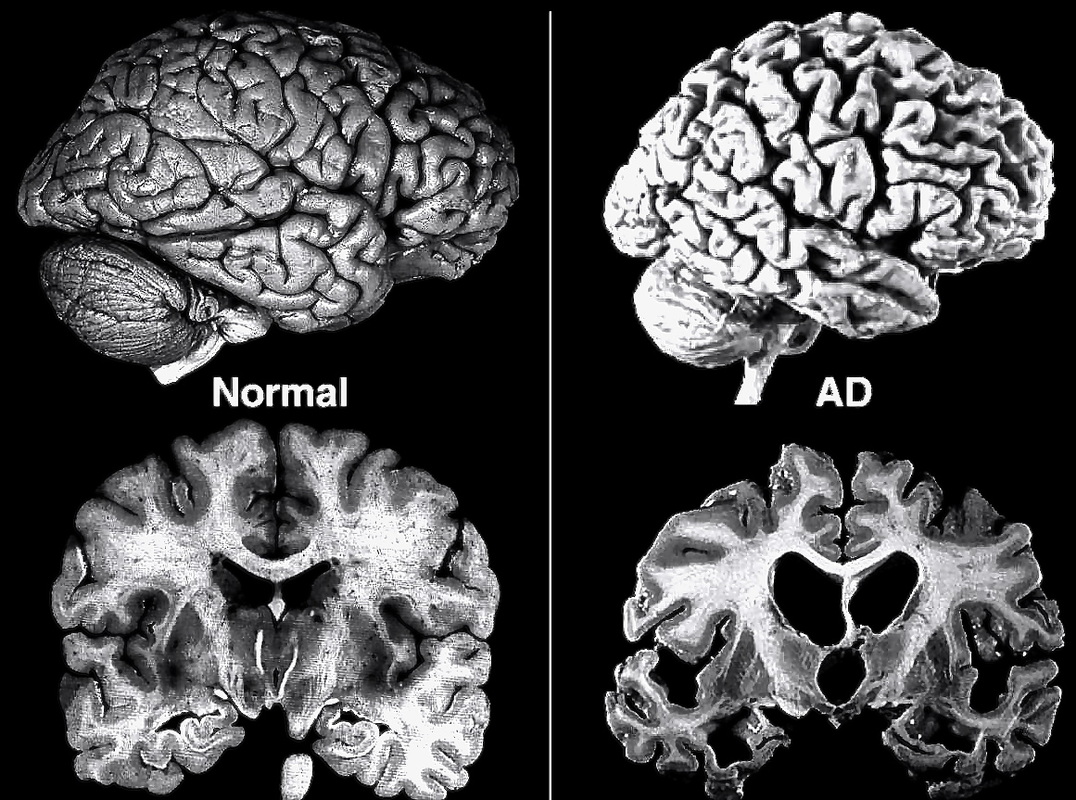
Loss of brain tissue in patients with Alzheimer's disease
Aphasia sub-types: basic dichotomy
Despite there being many different aphasia variations, they all can be roughly divided in two basic categories: Broca's and Wernicke's aphasias. Pierre Paul Broca (1824-1880) famously studied a patient Leborgne known as 'Tan' who could not say much more than this word, 'tan'. When the patient died, Broca performed an autopsy and located the damaged area, now known as a Broca's area. He made a picture, too; here it is:

Tan's brain with a damaged Broca's area
A bit later, in 1874, Carl Wernicke (1848-1904) described a patient who, on the contrary, had troubles comprehending language, who had a lesion in a more posterior region. He could produce long sentences with difficult grammar, however his speech would not make much sense - and he could not understand others, neither. Wernicke was the first one to differentiate between the two different types of aphasia.
Now, these sub-types are most commonly known as Broca and Wernicke aphasias, but terminology varies widely in literature, for example:
- Motor v Sensory
- Anterior v Posterior
- Syntactic v Semantic
- Grammar v Lexicon
- Rule-based b Memory-based aphasia
- etc.
So, really, what are the key symptoms for each of these sub-types?
Broca's aphasia
1. Difficulty producing sentences. The patients sometimes can say some very basic ones, which do not involve almost any grammar, such as 'want drink', or 'go bed'.
2. Ability to write is often impaired
3. May understand speech, but have difficulty with grammar. For example, they will struggle to see the difference between ' I gave book to my friend' and 'My friend game me the book'.
4. Comprehension of written speech may be also affected; the patients sometimes struggle to 'sound' written words in their heads.
Wernicke's aphasia
1. The patients would be able to produce sentences with complex grammar, however the ones which would not make sense due to the wrong usage of words. For example, they might say 'That was just like time for the next week when the bait'. Sometimes the same occurs in their written speech.
2. Those with Wernicke's aphasia would often not realise that what they are saying does not make sense, and get angry with people struggling to understand them.
3. Have difficulty understanding other people.
Now, these sub-types are most commonly known as Broca and Wernicke aphasias, but terminology varies widely in literature, for example:
- Motor v Sensory
- Anterior v Posterior
- Syntactic v Semantic
- Grammar v Lexicon
- Rule-based b Memory-based aphasia
- etc.
So, really, what are the key symptoms for each of these sub-types?
Broca's aphasia
1. Difficulty producing sentences. The patients sometimes can say some very basic ones, which do not involve almost any grammar, such as 'want drink', or 'go bed'.
2. Ability to write is often impaired
3. May understand speech, but have difficulty with grammar. For example, they will struggle to see the difference between ' I gave book to my friend' and 'My friend game me the book'.
4. Comprehension of written speech may be also affected; the patients sometimes struggle to 'sound' written words in their heads.
Wernicke's aphasia
1. The patients would be able to produce sentences with complex grammar, however the ones which would not make sense due to the wrong usage of words. For example, they might say 'That was just like time for the next week when the bait'. Sometimes the same occurs in their written speech.
2. Those with Wernicke's aphasia would often not realise that what they are saying does not make sense, and get angry with people struggling to understand them.
3. Have difficulty understanding other people.
Treatments
1. Speech and Language Therapy (SLT) is the most commonly used treatment method. It aims to do three things mainly: help to relearn lost communication skills if it is possible, make the best use of the abilities which are still intact and learn new ways of communication. It has been shown that intensive course of SLT (say, 10 hours per week for couple of months) is much more effective than just couple of hours per week for a longer period. It is also important to make the therapy personalised, as the patients are much more responsive when working with names/photographs which they relate to. Group therapy among the other patients with aphasia might be very beneficial, as it encourages communication with different people and decreases the possible feeling of isolation. There are several SLT techniques which can be used depending on the type and severity of the condition, as well as patient's preference.
- Promoting Aphasics' Communicative Effectiveness (PACE)
This technique encourages patients to engage into conversation using any ways of communication by starting from a simple topic (for example, descriptions of a patient's relative or friend) and gradually moving on to more complex ones - such as discussion of movies and patient's hobbies. The technique often involves usage of pictures and photographs to stimulate a conversation.
- Melodic intonation therapy (MIT)
MIT is based on the fact that the majority of people with Broca aphasia, who can not produce language, can still sing. This therapy involves patients humming or singing phrases or words which they have difficulty with pronouncing. The therapy was shown to increase the number of words a person can recall.
- Constraint-induced aphasia therapy (CIAT)
CIAT is used with patients with chronic, long-term aphasia. Such patients often develop compensatory strategies for communication, such as simple pointing and gesturing (instead of learning sig language) and producing imitation sounds - such as 'shhhhhh' for 'wind'. Usage of these strategies often leads to further loss of communication skills. CIAT aims to detect them and to encourage patients to learn new, more complex communication methods that force the brain to make use of its language centre, such as drawing or using communication tools, such as a speech synthesiser.
2. Transcranial stimulation is a new method of treatment, and at the moment is only used in clinical trials. It has been shown to stimulate damaged areas of the language centre and help those with aphasia to improve their ability to remember certain names of people, places and objects. There are two types:
- Transcranial direct current stimulation (tDCS)
Electrodes (small metallic discs) are placed on the surface of the scalp and a small electrical current is passed through them
- Transcranial magnetic stimulation (TMS)
Magnetic coils are placed above the scalp which create short-lasting electrical currents in the brain below the stimulation site
3. Medications for aphasia treatment are not yet available outside the clinical trials neither. However, researchers are now studying two drugs which could potentially help those with aphasia.
- Bromocriptine
It is thought it may help stimulate certain areas of the brain’s language centre.
- Donepezil
Increases levels of a chemical called acetylcholine in the brain. This is thought to lead to an increase in cognitive ability (the ability to think, reason and plan). The drug has been proved effective in improving the ability to name objects, people and places correctly.
- Promoting Aphasics' Communicative Effectiveness (PACE)
This technique encourages patients to engage into conversation using any ways of communication by starting from a simple topic (for example, descriptions of a patient's relative or friend) and gradually moving on to more complex ones - such as discussion of movies and patient's hobbies. The technique often involves usage of pictures and photographs to stimulate a conversation.
- Melodic intonation therapy (MIT)
MIT is based on the fact that the majority of people with Broca aphasia, who can not produce language, can still sing. This therapy involves patients humming or singing phrases or words which they have difficulty with pronouncing. The therapy was shown to increase the number of words a person can recall.
- Constraint-induced aphasia therapy (CIAT)
CIAT is used with patients with chronic, long-term aphasia. Such patients often develop compensatory strategies for communication, such as simple pointing and gesturing (instead of learning sig language) and producing imitation sounds - such as 'shhhhhh' for 'wind'. Usage of these strategies often leads to further loss of communication skills. CIAT aims to detect them and to encourage patients to learn new, more complex communication methods that force the brain to make use of its language centre, such as drawing or using communication tools, such as a speech synthesiser.
2. Transcranial stimulation is a new method of treatment, and at the moment is only used in clinical trials. It has been shown to stimulate damaged areas of the language centre and help those with aphasia to improve their ability to remember certain names of people, places and objects. There are two types:
- Transcranial direct current stimulation (tDCS)
Electrodes (small metallic discs) are placed on the surface of the scalp and a small electrical current is passed through them
- Transcranial magnetic stimulation (TMS)
Magnetic coils are placed above the scalp which create short-lasting electrical currents in the brain below the stimulation site
3. Medications for aphasia treatment are not yet available outside the clinical trials neither. However, researchers are now studying two drugs which could potentially help those with aphasia.
- Bromocriptine
It is thought it may help stimulate certain areas of the brain’s language centre.
- Donepezil
Increases levels of a chemical called acetylcholine in the brain. This is thought to lead to an increase in cognitive ability (the ability to think, reason and plan). The drug has been proved effective in improving the ability to name objects, people and places correctly.
An alternative view worth mentioning
Nowadays, aphasia is commonly seen as an impairment of language function, which does not affect cognition per se. However, it is important to note that there is another school of thought which views aphasia as a deeper impairment of thought processes. For example, Broca (1869) suggested that loss of language comprehension was caused by decline of intelligence. Finkelnburg (1870) saw aphasia as loss of ability to comprehend the significance of learned symbols and signs, and called it asymbolia. Finally, for Hughlings Jackson (1964), aphasia was defined as a loss of an ability to build propositions (i.e. statements): that is, to express original ideas in creatively generated forms. To him, propositions are opposed to automatic utterances - such as swearing, automatic counting, greetings - or repeating a word 'tan'.
 RSS Feed
RSS Feed
