

Dementia is a gradual decline in brain's functioning. It causes a number of symptoms that interfere with a person's ability to carry out the normal tasks of daily living. These may include:
- Memory disruption
- Changes in mood and/or personality
- Decreased cognitive ability
- Affected Theory of Mind ability (ability to understand others' mental states)
In this post, I will describe such types of dementia as Alzheimer's disease, vascular dementia and several subtypes of FTD (Frontotemporal dementia).
- Memory disruption
- Changes in mood and/or personality
- Decreased cognitive ability
- Affected Theory of Mind ability (ability to understand others' mental states)
In this post, I will describe such types of dementia as Alzheimer's disease, vascular dementia and several subtypes of FTD (Frontotemporal dementia).
Alzheimer's disease
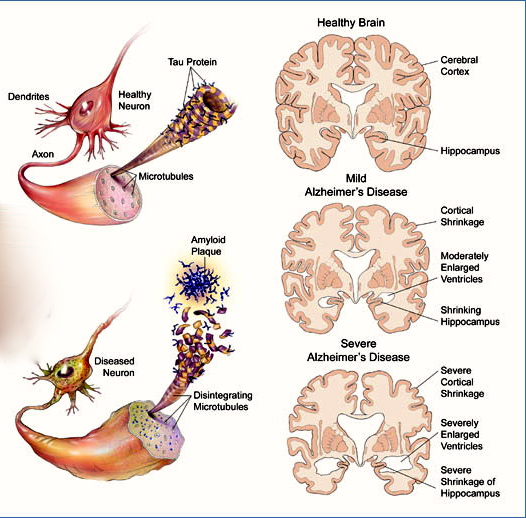
AD is the most common type of dementia, however the cause of the disease remains unknown. What happens is affected neurons disintegrate, causing the formation of protein deposits called 'amyloid plaques' (outside the neurons) and tangles (inside the neurons). These cause the cells around to die, affecting person's memory and overall cognitive ability; mid-brain (hippocampus) is normally affected first, and then the disease spreads further. Usually occipital lobes stay intact, however some AD types do affect those areas as well.
Mostly it is people over 65 who suffer from AD, however it does affect younger people too - especially when there is a family history of a disease.
Mostly it is people over 65 who suffer from AD, however it does affect younger people too - especially when there is a family history of a disease.
Vascular dementia
- Vascular dementia develops when the arteries supplying blood to the brain tissues become blocked. This disrupts the supply of oxygen and nutrients to the cells, which leads to very small strokes as tiny areas of the brain are damaged in this way. Vascular dementia often progresses in a step-wise fashion.
Many people with dementia have a combination of Alzheimer's disease and vascular dementia - this is known as mixed.
FTD
Frontotemporal dementia (FTD) is characterised by a slow loss of cognitive function caused by atrophy in frontal and temporal lobe, with occipital and parietal lobes typically staying intact. It is a second to AD in prevalence among the causes of dementia (around 20% of cases). FTD might be caused by Pick's disease: a disease which causes nerve cells to die. It results from the diseased tau proteins clustering into aggregations known as Pick bodies.
FTD is different from the AD, as it typically leaves memory unaffected, disrupting person's behaviour, social conduct, personality and ability to regulate emotions. FTDs can be subdivided as follows:
1. Behavioural variant (bvFTD)
Behavioural variant of the FTD causes slowly progressing changes in one's behaviour. These can make a patient either apathetic or disinhibited. Apathetic patients tend to withdraw from society and dramatically decrease levels of any activity. Disinhibited ones make inappropriate (often sexual) comments and act inappropriately in social situations. Personality traits often change, as do eating habits; patients often become really keen on sweets.
bvFTD is hard to detect on early stages, as there is no subjective complaints; patients usually don't feel there is anything wrong. It is normally relatives and friends who notice changes in one's behaviour and seek medical advice. However even then MRIs and MMSEs might not be able to detect any abnormalities if the desease is on early stage.
So how do you detect the bvFTD in its early stages? There are couple of tests which were shown to be quite helpful. In general, BvFTD patients perform poorer on False Belief tasks of first order (e.g. Sally-Anne task) and Faux Pas tasks than the AD patients. Second order False Belief tasks, which demand more cognitive effort, are almost equally challenging for the AD and bvFTD patients - although, arguably, for different reasons.
2. Semantic dementia
Semantic dementia is characterised by declining knowledge of ordinary words. Usually, a person gradually degrades to general concepts over time. For example, an SD patient might still be able to name a horse at an early stage; in couple of years time, (s)he might identify it as an 'animal'; later might name it as a 'creature'. A good test which demonstrates this degradation is giving a patient a picture of, say, a pigeon, and asking him/her to copy it. With the picture present, the drawing is likely to be ok (depending on the one's drawing abilities). However, about 10 seconds after the picture is taken away, SD patient is likely to draw a pigeon with features of a typical animal, for example with four legs. It happens because the knowledge of what a 'pigeon' is is gone, while a concept of an 'animal' is still present in patient's memory.
Those with semantic dementia usually preserve episodic memory (unlike AD patients), which helps them to understand concepts even when they forget names for them. For example, they might not be able to name a horse anymore, but might describe it as 'I used to ride it as a kid'.
SD patients preserve complex emotions (which might not be the case with bvFTD patients) even though they might lack the words to describe them. They are typically better with verbs than nouns.
3. Progressive non-fluent aphasia
This disease is associated with a progressive impairment of speech production, with speech comprehension remaining intact. As the disease develops, speech quantity decreases and many patients become mute. Cognitive domains other than language are rarely affected early on. However, as the disease progresses other domains can get affected. Problems with writing, reading and speech comprehension can occur, as can behavioural features similar to FTD.
FTD is different from the AD, as it typically leaves memory unaffected, disrupting person's behaviour, social conduct, personality and ability to regulate emotions. FTDs can be subdivided as follows:
1. Behavioural variant (bvFTD)
Behavioural variant of the FTD causes slowly progressing changes in one's behaviour. These can make a patient either apathetic or disinhibited. Apathetic patients tend to withdraw from society and dramatically decrease levels of any activity. Disinhibited ones make inappropriate (often sexual) comments and act inappropriately in social situations. Personality traits often change, as do eating habits; patients often become really keen on sweets.
bvFTD is hard to detect on early stages, as there is no subjective complaints; patients usually don't feel there is anything wrong. It is normally relatives and friends who notice changes in one's behaviour and seek medical advice. However even then MRIs and MMSEs might not be able to detect any abnormalities if the desease is on early stage.
So how do you detect the bvFTD in its early stages? There are couple of tests which were shown to be quite helpful. In general, BvFTD patients perform poorer on False Belief tasks of first order (e.g. Sally-Anne task) and Faux Pas tasks than the AD patients. Second order False Belief tasks, which demand more cognitive effort, are almost equally challenging for the AD and bvFTD patients - although, arguably, for different reasons.
2. Semantic dementia
Semantic dementia is characterised by declining knowledge of ordinary words. Usually, a person gradually degrades to general concepts over time. For example, an SD patient might still be able to name a horse at an early stage; in couple of years time, (s)he might identify it as an 'animal'; later might name it as a 'creature'. A good test which demonstrates this degradation is giving a patient a picture of, say, a pigeon, and asking him/her to copy it. With the picture present, the drawing is likely to be ok (depending on the one's drawing abilities). However, about 10 seconds after the picture is taken away, SD patient is likely to draw a pigeon with features of a typical animal, for example with four legs. It happens because the knowledge of what a 'pigeon' is is gone, while a concept of an 'animal' is still present in patient's memory.
Those with semantic dementia usually preserve episodic memory (unlike AD patients), which helps them to understand concepts even when they forget names for them. For example, they might not be able to name a horse anymore, but might describe it as 'I used to ride it as a kid'.
SD patients preserve complex emotions (which might not be the case with bvFTD patients) even though they might lack the words to describe them. They are typically better with verbs than nouns.
3. Progressive non-fluent aphasia
This disease is associated with a progressive impairment of speech production, with speech comprehension remaining intact. As the disease develops, speech quantity decreases and many patients become mute. Cognitive domains other than language are rarely affected early on. However, as the disease progresses other domains can get affected. Problems with writing, reading and speech comprehension can occur, as can behavioural features similar to FTD.
 RSS Feed
RSS Feed
